How You Can Diagnose Pes Planus
Overview
Basically, fallen arches refers to a flattening of the feet that takes place in adulthood. Although there may be other causes, this flattening usually occurs when the tendon (posterior tibial tendon) and ligaments that hold the arch in place gradually stretch. As we get older and our cumulative use of these tendons and ligaments increases, they lose their ability to maintain that nice arch shape, and may even begin to tear. This stretching or tearing may also be the result of an injury, obesity, or a genetic predisposition for flat feet.
Causes
Having low or no arches is normal for some people. In these cases, flat feet are usually inherited and the feet are fairly flexible. Occasionally, flat feet can be caused by an abnormality that develops in the womb, such as a problem with a joint or where two or more bones are fused together. This is known as tarsal coalition and results in the feet being flat and stiff. Flat feet that develop in later life can be caused by a condition that affects the joints, such as arthritis, or an injury to a muscle, tendon or joint in the foot. Conditions that affect the nervous system (brain and spinal cord) can also cause the arches to fall. Over time, the muscles gradually become stiffer and weaker and lose their flexibility. Conditions where this can occur include cerebral palsy, spina bifida and muscular dystrophy. Adult-acquired flat feet often affect women over 40 years of age. It often goes undiagnosed and develops when the tendon that supports the foot arch gradually stretches over time. It's not fully understood what causes the tendon to become stretched, but some experts believe that wearing high heels and standing or walking for long periods may play a part. Obesity, high blood pressure (hypertension) and diabetes are all risk factors. Recent research has found a link with changes to the tendon in the foot and an increase in a type of protein called proteolytic enzyme. These enzymes can break down some areas of the tendon, weakening it and causing the foot arch to fall. Similar changes are also seen in other conditions, such as Achilles tendonitis. This could have important implications for treating flat feet because medication that specifically targets these enzymes could provide an alternative to surgery. However, further research is needed and this type of treatment is thought to be about 10 to 15 years away.
Symptoms
People will have a very heavily dropped arch and it won?t affect them at all and people will have it slightly dropped and it could cause fierce problems. It could cause things like plantar fasciitis, it could cause heel spurs, desperate ball-of-the-foot pressure, or pressure on the big toe known as the hallux which causes discomfort in the foot. It will create problems upwards to the knees, hips and the back once you?re out of line.
Diagnosis
Runners are often advised to get a gait analysis to determine what type of foot they have and so what kind of running shoe they require. This shouldn?t stop at runners. Anyone that plays sports could benefit from this assessment. Sports shoes such as football boots, astro trainers and squash trainers often have very poor arch support and so for the 60-80% of us who do overpronate or have flat feet they are left unsupported. A change of footwear or the insertion of arch support insoles or orthotics can make a massive difference to your risk of injury, to general aches and pains and even to your performance.
How do you get an arch in your foot?
Non Surgical Treatment
The type of treatment will depend on the stage of PTTD present. There are four stages of posterior tibial tendon dysfunction. Stage I. The posterior tibial tendon is inflamed but has normal strength. There is little to no change in the arch of the foot. The patient can still perform a single-limb heel rise and has a flexible hindfoot. Orthotic treatment options include modified off the shelf inserts and custom molded orthotics. Stage 2. The tendon is partially torn or shows degenerative changes and as a result loses strength.There is considerable flattening of the arch without arthritic changes in the foot. The patient cannot perform single-limb heel rise. Pain is now present on the lateral aspect of the ankle. Orthotic treatment is similar as that in stage I, with the addition of more rigid arch supports and wedging. Stage 3. Results when the posterior tibial tendon is torn and not functioning. As a result the arch is completely collapsed with arthritic changes in the foot. A solid ankle AFO is suggested in conjunction with a modified orthopedic shoe. Stage 4. Is identical to stage three except that the ankle joint also becomes arthritic. A rigid AFO and modified orthopedic shoe is required.
Surgical Treatment

This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
Sit up straight in a chair with your feet flat on the ground. Scrunch up the toes of one foot as if you are trying to grab hold of the floor then use your toes to drag your foot a small distance forwards. Do this a couple of times on each foot, but don?t use your leg muscles to push your foot forward -- the movement should come solely from the muscles in your feet. Sit in a chair and place a cleaning cloth, towel or small ball on the floor at your feet. Use the toes of one foot to grasp the object and lift it off the floor. This action will require you to clench your toes and contract your arch. Once you have lifted the object a little way off the floor, try to throw it in the air and catch it by stretching your toes and arch out and upwards. Repeat the exercise several times on both feet. Sit on the floor with your legs straight out in front of you then bend your knees out to either side and place the soles of your feet together so your legs form a diamond. Hold on to your ankles and, keeping your heels together at all times, separate your feet so your toes point out to either side. Open and close your feet in this way several times, making sure your little toes stay in contact with the floor throughout the exercise. Starting in the same position, try separating your heels, keeping your toes together at all times.
Basically, fallen arches refers to a flattening of the feet that takes place in adulthood. Although there may be other causes, this flattening usually occurs when the tendon (posterior tibial tendon) and ligaments that hold the arch in place gradually stretch. As we get older and our cumulative use of these tendons and ligaments increases, they lose their ability to maintain that nice arch shape, and may even begin to tear. This stretching or tearing may also be the result of an injury, obesity, or a genetic predisposition for flat feet.
Causes
Having low or no arches is normal for some people. In these cases, flat feet are usually inherited and the feet are fairly flexible. Occasionally, flat feet can be caused by an abnormality that develops in the womb, such as a problem with a joint or where two or more bones are fused together. This is known as tarsal coalition and results in the feet being flat and stiff. Flat feet that develop in later life can be caused by a condition that affects the joints, such as arthritis, or an injury to a muscle, tendon or joint in the foot. Conditions that affect the nervous system (brain and spinal cord) can also cause the arches to fall. Over time, the muscles gradually become stiffer and weaker and lose their flexibility. Conditions where this can occur include cerebral palsy, spina bifida and muscular dystrophy. Adult-acquired flat feet often affect women over 40 years of age. It often goes undiagnosed and develops when the tendon that supports the foot arch gradually stretches over time. It's not fully understood what causes the tendon to become stretched, but some experts believe that wearing high heels and standing or walking for long periods may play a part. Obesity, high blood pressure (hypertension) and diabetes are all risk factors. Recent research has found a link with changes to the tendon in the foot and an increase in a type of protein called proteolytic enzyme. These enzymes can break down some areas of the tendon, weakening it and causing the foot arch to fall. Similar changes are also seen in other conditions, such as Achilles tendonitis. This could have important implications for treating flat feet because medication that specifically targets these enzymes could provide an alternative to surgery. However, further research is needed and this type of treatment is thought to be about 10 to 15 years away.
Symptoms
People will have a very heavily dropped arch and it won?t affect them at all and people will have it slightly dropped and it could cause fierce problems. It could cause things like plantar fasciitis, it could cause heel spurs, desperate ball-of-the-foot pressure, or pressure on the big toe known as the hallux which causes discomfort in the foot. It will create problems upwards to the knees, hips and the back once you?re out of line.
Diagnosis
Runners are often advised to get a gait analysis to determine what type of foot they have and so what kind of running shoe they require. This shouldn?t stop at runners. Anyone that plays sports could benefit from this assessment. Sports shoes such as football boots, astro trainers and squash trainers often have very poor arch support and so for the 60-80% of us who do overpronate or have flat feet they are left unsupported. A change of footwear or the insertion of arch support insoles or orthotics can make a massive difference to your risk of injury, to general aches and pains and even to your performance.
How do you get an arch in your foot?
Non Surgical Treatment
The type of treatment will depend on the stage of PTTD present. There are four stages of posterior tibial tendon dysfunction. Stage I. The posterior tibial tendon is inflamed but has normal strength. There is little to no change in the arch of the foot. The patient can still perform a single-limb heel rise and has a flexible hindfoot. Orthotic treatment options include modified off the shelf inserts and custom molded orthotics. Stage 2. The tendon is partially torn or shows degenerative changes and as a result loses strength.There is considerable flattening of the arch without arthritic changes in the foot. The patient cannot perform single-limb heel rise. Pain is now present on the lateral aspect of the ankle. Orthotic treatment is similar as that in stage I, with the addition of more rigid arch supports and wedging. Stage 3. Results when the posterior tibial tendon is torn and not functioning. As a result the arch is completely collapsed with arthritic changes in the foot. A solid ankle AFO is suggested in conjunction with a modified orthopedic shoe. Stage 4. Is identical to stage three except that the ankle joint also becomes arthritic. A rigid AFO and modified orthopedic shoe is required.
Surgical Treatment
This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients.
Prevention
Sit up straight in a chair with your feet flat on the ground. Scrunch up the toes of one foot as if you are trying to grab hold of the floor then use your toes to drag your foot a small distance forwards. Do this a couple of times on each foot, but don?t use your leg muscles to push your foot forward -- the movement should come solely from the muscles in your feet. Sit in a chair and place a cleaning cloth, towel or small ball on the floor at your feet. Use the toes of one foot to grasp the object and lift it off the floor. This action will require you to clench your toes and contract your arch. Once you have lifted the object a little way off the floor, try to throw it in the air and catch it by stretching your toes and arch out and upwards. Repeat the exercise several times on both feet. Sit on the floor with your legs straight out in front of you then bend your knees out to either side and place the soles of your feet together so your legs form a diamond. Hold on to your ankles and, keeping your heels together at all times, separate your feet so your toes point out to either side. Open and close your feet in this way several times, making sure your little toes stay in contact with the floor throughout the exercise. Starting in the same position, try separating your heels, keeping your toes together at all times.
Treatment For Apparent Leg Length Discrepancy
Overview
Have you ever been told or noticed that one of your legs is a bit longer than the other? Do you have incidences of lower back pain? These two things could be related. Most individuals have a small difference in their leg lengths. For some, the discrepancy is small and negligible and will not be a contributor to lower back pain. This is usually the case for people if their leg length is less than 5 millimeters. However, a difference of leg lengths greater than 5 millimeters (1/4 inch) can contribute to lower back pain. If you have a leg length difference of greater than 9 mm, then you have a 6X greater likelihood of having an episode of lower back pain.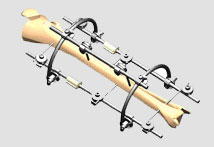
Causes
A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences.
Symptoms
The symptoms of limb deformity can range from a mild difference in the appearance of a leg or arm to major loss of function of the use of an extremity. For instance, you may notice that your child has a significant limp. If there is deformity in the extremity, the patient may develop arthritis as he or she gets older, especially if the lower extremities are involved. Patients often present due to the appearance of the extremity (it looks different from the other side).
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.

shoe lifts for women's shoes
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Have you ever been told or noticed that one of your legs is a bit longer than the other? Do you have incidences of lower back pain? These two things could be related. Most individuals have a small difference in their leg lengths. For some, the discrepancy is small and negligible and will not be a contributor to lower back pain. This is usually the case for people if their leg length is less than 5 millimeters. However, a difference of leg lengths greater than 5 millimeters (1/4 inch) can contribute to lower back pain. If you have a leg length difference of greater than 9 mm, then you have a 6X greater likelihood of having an episode of lower back pain.
Causes
A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences.
Symptoms
The symptoms of limb deformity can range from a mild difference in the appearance of a leg or arm to major loss of function of the use of an extremity. For instance, you may notice that your child has a significant limp. If there is deformity in the extremity, the patient may develop arthritis as he or she gets older, especially if the lower extremities are involved. Patients often present due to the appearance of the extremity (it looks different from the other side).
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.
shoe lifts for women's shoes
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
All You Might Want To Know About Heel Discomfort
Overview

Heel pain is a very common condition treated in our podiatric office. Patients come in complaining of pain to the bottom of their heel, sometimes radiating into the arch area and are seeking effective treatment. Dr. Weinert often speaks with patients who thought their heel pain would just go away on its own. However, with conditions such as heel spur syndrome or plantar fasciitis, this often is not the case. If heel pain is not treated properly, symptoms will only get worse for the patient and can result in further pain and disability. This can happen not only in the foot, but in the ankle, knee, hip, lower back and even up in to the shoulder areas as well. The foot is the foundation for the whole body system and if the foot or the heel hurts, then you can feel pain all over. Foot health starts with knowing the causes of heel pain and symptoms to look out for. Early intervention will prevent further damage to the feet and Dr. Weinert offers several treatment options to help his patients suffering with heel pain.
Causes
The most common cause of heel pain in adults is plantar fasciitis, which is an inflammation of the band of tissue in the sole that connects the heel to the toes and forms the natural foot arch. Plantar fasciitis may or may not be complicated by a calcaneal spur, a small bone growth that protrudes out of the heel. Plantar fasciitis may also be referred to as plantar fasciosis. In contrast to fasciitis, which essentially means inflammation, fasciosis refers to degeneration of the tissue. In fact, if left untreated, acute plantar fasciitis may develop into a chronic painful condition, which results in slow and irreversible degeneration of the fascia, hence plantar fasciosis. The location of the pain is usually exactly under the heel but may also occur in the arch of the foot. Pain typical to plantar fasciitis is that which feels worse when arising on to your feet such as in mornings or after sitting down for a while, and usually progresses in severity when left untreated.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
Your GP or podiatrist (a healthcare professional who specialises in foot care) may be able to diagnose the cause of your heel pain by asking about your symptoms and examining your heel and foot. You will usually only need further tests if you have additional symptoms that suggest the cause of your heel pain is not inflammation, such as numbness or a tingling sensation in your foot - this could be a sign of nerve damage in your feet and legs (peripheral neuropathy), your foot feels hot and you have a high temperature (fever) of 38C (100.4F) or above - these could be signs of a bone infection, you have stiffness and swelling in your heel - this could be a sign of arthritis. Possible further tests may include, blood tests, X-rays - where small doses of radiation are used to detect problems with your bones and tissues, a magnetic resonance imaging (MRI) scan or ultrasound scan, which are more detailed scans.
Non Surgical Treatment
Heel pain often goes away on its own with home care. For heel pain that isn't severe, try the following. Rest. If possible, avoid activities that put stress on your heels, such as running, standing for long periods or walking on hard surfaces. Ice. Place an ice pack or bag of frozen peas on your heel for 15 to 20 minutes three times a day. New shoes. Be sure your shoes fit properly and provide plenty of support. If you're an athlete, choose shoes appropriate for your sport and replace them regularly. Foot supports. Heel cups or wedges that you buy in the drugstore often provide relief. Custom-made orthotics usually aren't needed for heel problems. Over-the-counter pain medications. Aspirin or ibuprofen (Advil, Motrin IB, others) can reduce inflammation and pain.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
Where is a heel spur located?
Prevention

It may not be possible to prevent all cases of heel pain. However, there are some easy steps that you can take to avoid injury to the heel and prevent pain. Whenever possible, you should wear shoes that fit properly and support the foot, wear the right shoes for physical activity, stretch your muscles before exercising, pace yourself during physical activity, maintain a healthy diet, rest when you feel tired or when your muscles ache, maintain a healthy weight.
Heel pain is a very common condition treated in our podiatric office. Patients come in complaining of pain to the bottom of their heel, sometimes radiating into the arch area and are seeking effective treatment. Dr. Weinert often speaks with patients who thought their heel pain would just go away on its own. However, with conditions such as heel spur syndrome or plantar fasciitis, this often is not the case. If heel pain is not treated properly, symptoms will only get worse for the patient and can result in further pain and disability. This can happen not only in the foot, but in the ankle, knee, hip, lower back and even up in to the shoulder areas as well. The foot is the foundation for the whole body system and if the foot or the heel hurts, then you can feel pain all over. Foot health starts with knowing the causes of heel pain and symptoms to look out for. Early intervention will prevent further damage to the feet and Dr. Weinert offers several treatment options to help his patients suffering with heel pain.
Causes
The most common cause of heel pain in adults is plantar fasciitis, which is an inflammation of the band of tissue in the sole that connects the heel to the toes and forms the natural foot arch. Plantar fasciitis may or may not be complicated by a calcaneal spur, a small bone growth that protrudes out of the heel. Plantar fasciitis may also be referred to as plantar fasciosis. In contrast to fasciitis, which essentially means inflammation, fasciosis refers to degeneration of the tissue. In fact, if left untreated, acute plantar fasciitis may develop into a chronic painful condition, which results in slow and irreversible degeneration of the fascia, hence plantar fasciosis. The location of the pain is usually exactly under the heel but may also occur in the arch of the foot. Pain typical to plantar fasciitis is that which feels worse when arising on to your feet such as in mornings or after sitting down for a while, and usually progresses in severity when left untreated.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
Your GP or podiatrist (a healthcare professional who specialises in foot care) may be able to diagnose the cause of your heel pain by asking about your symptoms and examining your heel and foot. You will usually only need further tests if you have additional symptoms that suggest the cause of your heel pain is not inflammation, such as numbness or a tingling sensation in your foot - this could be a sign of nerve damage in your feet and legs (peripheral neuropathy), your foot feels hot and you have a high temperature (fever) of 38C (100.4F) or above - these could be signs of a bone infection, you have stiffness and swelling in your heel - this could be a sign of arthritis. Possible further tests may include, blood tests, X-rays - where small doses of radiation are used to detect problems with your bones and tissues, a magnetic resonance imaging (MRI) scan or ultrasound scan, which are more detailed scans.
Non Surgical Treatment
Heel pain often goes away on its own with home care. For heel pain that isn't severe, try the following. Rest. If possible, avoid activities that put stress on your heels, such as running, standing for long periods or walking on hard surfaces. Ice. Place an ice pack or bag of frozen peas on your heel for 15 to 20 minutes three times a day. New shoes. Be sure your shoes fit properly and provide plenty of support. If you're an athlete, choose shoes appropriate for your sport and replace them regularly. Foot supports. Heel cups or wedges that you buy in the drugstore often provide relief. Custom-made orthotics usually aren't needed for heel problems. Over-the-counter pain medications. Aspirin or ibuprofen (Advil, Motrin IB, others) can reduce inflammation and pain.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
Where is a heel spur located?
Prevention
It may not be possible to prevent all cases of heel pain. However, there are some easy steps that you can take to avoid injury to the heel and prevent pain. Whenever possible, you should wear shoes that fit properly and support the foot, wear the right shoes for physical activity, stretch your muscles before exercising, pace yourself during physical activity, maintain a healthy diet, rest when you feel tired or when your muscles ache, maintain a healthy weight.
What Is Mortons Neuroma
Overview
 Morton?s neuroma is inflammation, thickening, or enlargement of the nerve between the bones of the toes (metatarsal bones). The condition is also called intermetatarsal neuroma. The thickening is usually found between bones of the third and fourth toes of the foot, but sometimes it may develop between the second and third toes. It occurs when the medial plantar nerve near the bones of those toes becomes compressed or irritated, possibly because the metatarsal bones press against the nerve in the narrow gap between the toes. If left untreated, Morton?s neuroma can cause a sharp, burning, or shooting pain that often gets worse over time. The pain becomes worse when a person walks or stands on the ball of the foot. Sometimes the pain reaches the toes next to the neuroma and a sensation of tingling or numbness is felt.
Morton?s neuroma is inflammation, thickening, or enlargement of the nerve between the bones of the toes (metatarsal bones). The condition is also called intermetatarsal neuroma. The thickening is usually found between bones of the third and fourth toes of the foot, but sometimes it may develop between the second and third toes. It occurs when the medial plantar nerve near the bones of those toes becomes compressed or irritated, possibly because the metatarsal bones press against the nerve in the narrow gap between the toes. If left untreated, Morton?s neuroma can cause a sharp, burning, or shooting pain that often gets worse over time. The pain becomes worse when a person walks or stands on the ball of the foot. Sometimes the pain reaches the toes next to the neuroma and a sensation of tingling or numbness is felt.
Causes
Experts are not sure what exactly causes Morton's neuroma. It seems to develop as a result of irritation, pressure or injury to one of the digital nerves that lead to the toes, which triggers a body response, resulting in thickened nerve tissue (neuroma). Feet conditions/situations that can cause the bones to rub against a nerve include high-heeled shoes, especially those over 2 inches (5cm), or a pointed or tight toe box which squash the toes together. This is probably why the condition is much more common in females than in males. High-arched foot, people whose feet have high arches are much more likely to suffer from Morton's neuroma than others. Flat feet, the arch of the foot collapses. The entire sole of the foot comes into complete or near-complete contact with the ground. A bunion, a localized painful swelling at the base of the big toe, which enlarges the joint. Hammer toe, a deformity of the proximal interphalangeal joint of the second, third, or fourth toe causing it to be permanently bent. Some high-impact sporting activities including running, karate, and court sports. Any sport that places undue pressure on the feet. Injuries, an injury or other type of trauma to the foot may lead to a neuroma.
Symptoms
You may initially experience a tingling sensation in the space between your toes, which gets worse over time. This leads to cramp in your toes and a sharp shooting or burning pain on the ball of your foot or at the base of your toes. The pain is often worse when walking or wearing shoes that press on the affected area. This is caused by irritation of the nerve between your toe bones (metatarsal bones). The tingling will eventually lead to pain, which can get worse over time. You may also experience cramping of your toes. The pain is usually felt as a sharp shooting or burning pain on the ball of the foot or at the base of the toes, which is often made worse when you're walking. Some people with Morton's neuroma feel anxious about walking or even placing their foot on the ground. The pain is likely to be more intense if you wear tight shoes, so wearing shoes that have more room in the toe area can help. Rubbing your foot may also lessen the pain.
Diagnosis
Based on the physical examination, your doctor usually can diagnose a Morton's neuroma without additional testing. A foot X-ray may be ordered to make sure that there isn't a stress fracture, but it will not show the actual neuroma. If the diagnosis is in doubt, your doctor may request magnetic resonance imaging (MRI) of the foot.
Non Surgical Treatment
Depending on your overall health, symptoms and severity of the neuroma, the condition may be treated conservatively and/or with surgery. Non-surgical methods for neuroma are aimed at decreasing and/or eliminating symptoms (pain). Wear proper supportive shoes. Use an arch support. Wear shoes with a wide toe box. Modify your activities. Lose weight. Wear shoes with cushion. Prescribe an oral anti-inflammatory medication. Anti-inflammatory medication is useful to significantly reduce pain and inflammation. A physical therapist may perform ultrasound and other techniques to reduce inflammation. You will also be instructed how to stretch your foot and leg properly. Padding and/or cushioning of the ball of the foot is an effective method of preventing physical irritation with shoes. A custom foot orthotic is a doctor prescribed arch support that is made directly from a casting (mold) of your feet, and theoretically should provide superior support compared to shoe insert that you would purchase from a pharmacy. A cortisone injection is a powerful anti-inflammatory medication that is used to rapidly reduce the pain associated with an inflamed nerve. The pain relief that you may experience from the injection(s) is often temporary. Typically injection(s) are administered once every 2 months for a total of 3 injections or until the pain is resolved. A sclerosing alcohol injection is placed around the involved nerve to weaken its capacity to report pain. In other words, the alcohol injection will ?deaden? the affected nerve. The pain relief that you may experience from the injection(s) can be permanent. Typically injection(s) are administered once every week for a few weeks until the pain is resolved.
Surgical Treatment
Surgery for neuroma most often involves removing affected nerve in the ball of the foot. An incision is made on the top of the foot and the nerve is carefully removed. Surgeon must remove the nerve far enough back so that the nerve doesn?t continue to become impinged at the ball of the foot. Alternatitvely, another type of surgery involves releasing a tight ligament that encases the nerve. Recovery after Morton?s neuroma (neurectomy) surgery is generally quick. Typically patients are walking on the operated foot in a post-surgical shoe for 2 - 4 weeks, depending on healing. Return to shoes is 2-6 weeks after the surgery. Factors that may prolong healing are age, smoking, poor nutritional status, and some medical problems.
Morton?s neuroma is inflammation, thickening, or enlargement of the nerve between the bones of the toes (metatarsal bones). The condition is also called intermetatarsal neuroma. The thickening is usually found between bones of the third and fourth toes of the foot, but sometimes it may develop between the second and third toes. It occurs when the medial plantar nerve near the bones of those toes becomes compressed or irritated, possibly because the metatarsal bones press against the nerve in the narrow gap between the toes. If left untreated, Morton?s neuroma can cause a sharp, burning, or shooting pain that often gets worse over time. The pain becomes worse when a person walks or stands on the ball of the foot. Sometimes the pain reaches the toes next to the neuroma and a sensation of tingling or numbness is felt.Causes
Experts are not sure what exactly causes Morton's neuroma. It seems to develop as a result of irritation, pressure or injury to one of the digital nerves that lead to the toes, which triggers a body response, resulting in thickened nerve tissue (neuroma). Feet conditions/situations that can cause the bones to rub against a nerve include high-heeled shoes, especially those over 2 inches (5cm), or a pointed or tight toe box which squash the toes together. This is probably why the condition is much more common in females than in males. High-arched foot, people whose feet have high arches are much more likely to suffer from Morton's neuroma than others. Flat feet, the arch of the foot collapses. The entire sole of the foot comes into complete or near-complete contact with the ground. A bunion, a localized painful swelling at the base of the big toe, which enlarges the joint. Hammer toe, a deformity of the proximal interphalangeal joint of the second, third, or fourth toe causing it to be permanently bent. Some high-impact sporting activities including running, karate, and court sports. Any sport that places undue pressure on the feet. Injuries, an injury or other type of trauma to the foot may lead to a neuroma.
Symptoms
You may initially experience a tingling sensation in the space between your toes, which gets worse over time. This leads to cramp in your toes and a sharp shooting or burning pain on the ball of your foot or at the base of your toes. The pain is often worse when walking or wearing shoes that press on the affected area. This is caused by irritation of the nerve between your toe bones (metatarsal bones). The tingling will eventually lead to pain, which can get worse over time. You may also experience cramping of your toes. The pain is usually felt as a sharp shooting or burning pain on the ball of the foot or at the base of the toes, which is often made worse when you're walking. Some people with Morton's neuroma feel anxious about walking or even placing their foot on the ground. The pain is likely to be more intense if you wear tight shoes, so wearing shoes that have more room in the toe area can help. Rubbing your foot may also lessen the pain.
Diagnosis
Based on the physical examination, your doctor usually can diagnose a Morton's neuroma without additional testing. A foot X-ray may be ordered to make sure that there isn't a stress fracture, but it will not show the actual neuroma. If the diagnosis is in doubt, your doctor may request magnetic resonance imaging (MRI) of the foot.
Non Surgical Treatment
Depending on your overall health, symptoms and severity of the neuroma, the condition may be treated conservatively and/or with surgery. Non-surgical methods for neuroma are aimed at decreasing and/or eliminating symptoms (pain). Wear proper supportive shoes. Use an arch support. Wear shoes with a wide toe box. Modify your activities. Lose weight. Wear shoes with cushion. Prescribe an oral anti-inflammatory medication. Anti-inflammatory medication is useful to significantly reduce pain and inflammation. A physical therapist may perform ultrasound and other techniques to reduce inflammation. You will also be instructed how to stretch your foot and leg properly. Padding and/or cushioning of the ball of the foot is an effective method of preventing physical irritation with shoes. A custom foot orthotic is a doctor prescribed arch support that is made directly from a casting (mold) of your feet, and theoretically should provide superior support compared to shoe insert that you would purchase from a pharmacy. A cortisone injection is a powerful anti-inflammatory medication that is used to rapidly reduce the pain associated with an inflamed nerve. The pain relief that you may experience from the injection(s) is often temporary. Typically injection(s) are administered once every 2 months for a total of 3 injections or until the pain is resolved. A sclerosing alcohol injection is placed around the involved nerve to weaken its capacity to report pain. In other words, the alcohol injection will ?deaden? the affected nerve. The pain relief that you may experience from the injection(s) can be permanent. Typically injection(s) are administered once every week for a few weeks until the pain is resolved.
Surgical Treatment
Surgery for neuroma most often involves removing affected nerve in the ball of the foot. An incision is made on the top of the foot and the nerve is carefully removed. Surgeon must remove the nerve far enough back so that the nerve doesn?t continue to become impinged at the ball of the foot. Alternatitvely, another type of surgery involves releasing a tight ligament that encases the nerve. Recovery after Morton?s neuroma (neurectomy) surgery is generally quick. Typically patients are walking on the operated foot in a post-surgical shoe for 2 - 4 weeks, depending on healing. Return to shoes is 2-6 weeks after the surgery. Factors that may prolong healing are age, smoking, poor nutritional status, and some medical problems.
Hammer Toe Cause & Therapy
 Overview
Overview
What are hammertoes, mallet toes and claw toes? Often the words are used interchangeably to mean an abnormally contracted toe like the drawing above. Technically speaking, a "Hammer Toe" is the name for a toe that is contracted at the first toe joint. If it's contracted at the second toe joint it is called a "mallet toe". IIf a toe is contracted at both toe joints, it is called a "claw toe". Each of these conditions can be quite uncomfortable and are cosmetically unappealing.
Causes
The constant pressure a woman's foot receives in high-heeled shoes due to the force of gravity causes their feet to naturally slide down and press on the lowest point of the shoe so they are not able to receive enough space and stretch out. The result is an eventual distortion of the woman's toes. The deformity comes as a result of the shortening of muscles inside the toes because the toes become used to being in a bent position, prompting the muscles to fail to extend any further and become tightened and curbed. At first, toes may still be stretched out if poor footwear is not being worn, yet if the habit is persistent...the person's toes will eventually become used to the position they are constantly in and muscle fibers inside them will harden and refuse to stretch. 
Symptoms
Here is a look at some of the symptoms hammertoe can cause. They include hammer-like or claw-like appearance of the toe. Pain when walking or moving the foot. Difficulty moving the toe. Corns may form on top of the toe. Callus may form on the sole of the foot. During the initial stages, you may be able to manually straighten your toe. This is called a flexible hammertoe. But as time passes, the toe will not move as easily and will continue to look like a hammer. Pressure and irritation over the joint can cause a blister to develop and become a corn over time. These corns have the potential to become infected and cause additional symptoms such as redness, bleeding, and difficulty wearing shoes and socks. Corns are the main cause of pain when hammertoes are developing.
Diagnosis
Some questions your doctor may ask of you include, when did you first begin having foot problems? How much pain are your feet or toes causing you? Where is the pain located? What, if anything, seems to improve your symptoms? What, if anything, appears to worsen your symptoms? What kind of shoes do you normally wear? Your doctor can diagnose hammertoe or mallet toe by examining your foot. Your doctor may also order X-rays to further evaluate the bones and joints of your feet and toes.
Non Surgical Treatment
If your hammertoe problem is diagnosed as flexible hammertoe, there are a number of nonsurgical treatments that may be able to straighten out your toe or toes and return them to their proper alignment. Padding and Taping. Your physician may pad the boney top-part of your hammertoe as a means of relieving pain, and may tape your toes as a way to change their position, correct the muscle imbalance and relieve the pressure that led to the hammertoe's development. Medication. Anti-inflammatory drugs such as aspirin and ibuprofen can help deal with inflammation, swelling and pain caused by your hammertoe. Cortisone injections may be prescribed for the same purpose. If your hammertoe is a consequence of arthritis, your physician may prescribe medications for that.
Surgical Treatment
For the surgical correction of a rigid hammertoe, the surgical procedure consists of removing the damaged skin where the corn is located. Then a small section of bone is removed at the level of the rigid joint. The sutures remain in place for approximately ten days. During this period of time it is important to keep the area dry. Most surgeons prefer to leave the bandage in place until the patient's follow-up visit, so there is no need for the patient to change the bandages at home. The patient is returned to a stiff-soled walking shoe in about two weeks. It is important to try and stay off the foot as much as possible during this time. Excessive swelling of the toe is the most common patient complaint. In severe cases of hammertoe deformity a pin may be required to hold the toe in place and the surgeon may elect to fuse the bones in the toe. This requires several weeks of recovery.
Bunions All The Things You Need To Learn
Overview
 What most people call a bunion is actually known as "Hallux valgus". Hallux valgus refers to the condition in which the big toe is angled excessively towards the second toe and a bunion is a symptom of the deformity. In a normal foot, the big toe and the long bone that leads up to it (the first metatarsal) are in a straight line. However, Hallux valgus occurs when the long foot bone veers towards your other foot and your big toes drifts towards your second toe. A bunion actually refers to the bony prominence on the side of the big toe. This can also form a large sac of fluid, known as a bursa, which can then become inflamed and sore.
What most people call a bunion is actually known as "Hallux valgus". Hallux valgus refers to the condition in which the big toe is angled excessively towards the second toe and a bunion is a symptom of the deformity. In a normal foot, the big toe and the long bone that leads up to it (the first metatarsal) are in a straight line. However, Hallux valgus occurs when the long foot bone veers towards your other foot and your big toes drifts towards your second toe. A bunion actually refers to the bony prominence on the side of the big toe. This can also form a large sac of fluid, known as a bursa, which can then become inflamed and sore.
Causes
There are many factors which can contribute to the development of a bunion. The common causes are genetic factors, poor foot mechanics, high-heeled or narrow footwear and trauma to the toe. It is believed that constant stress on the joint of the big toe causes mild displacement of the bones and the joint, along with thickening of the tissues and a change in the pull of the muscles. This can result in a degree of arthritis of the joint, and over time, further displacement of the toe. This may lead to pain, difficultly with fitting shoes and corns/calloused lesions due to excess pressure on the smaller digits.
Symptoms
Bunions are readily apparent, you can see the prominence at the base of the big toe or side of the foot. However, to fully evaluate your condition, the Podiatrist may take x-rays to determine the degree of the deformity and assess the changes that have occurred. Because bunions are progressive, they don't go away, and will usually get worse over time. But not all cases are alike, some bunions progress more rapidly than others. There is no clear-cut way to predict how fast a bunion will get worse. The severity of the bunion and the symptoms you have will help determine what treatment is recommended for you.
Diagnosis
Your family doctor or chiropodist /podiatrist can identify a bunion simply by examining your foot. During the exam, your big toe will be moved up and down to determine if your range of motion is limited. You will be examined for signs of redness or swelling and be questioned about your history of pain. A foot x-ray can show an abnormal angle between the big toe and the foot. In some cases, arthritis may also be seen. A X-ray of your foot may help identify the cause of the bunion and rate its severity.
Non Surgical Treatment
The treatment method your doctor chooses for you will be based on the severity of the bunion. Treatment can be simple and non-surgical or it can be complex, surgical, and costly. A bunion is permanent unless surgery is performed to remove it, but self-care can help to improve your symptoms. If you suspect that a bunion is developing, you should seek medical attention immediately. Here are the most common conservative treatment options. Changing your shoes. Adding custom orthotics to your shoes. Medication such as Tylenol for pain relief. Padding and taping to put your foot in its normal position. Applying ice or cold compresses to reduce swelling and pain. Keeping pressure off your affected toe, especially if there is swelling, redness, and pain. Before bed, separate the affected toe from the others with a foam-rubber pad and leave it there while you sleep. 
Surgical Treatment
To end persistent pain, your doctor may recommend a type of foot surgery called a bunionectomy to remove the bunion and perhaps to reshape the first toe joint. During the operation, the swollen tissue will be removed, the big toe will be straightened if necessary, and the bones of the affected joint may be reshaped or permanently joined. The goal of the surgery is to correct the cause of the bunion and to prevent the bunion from growing back. After surgery, pain medication will be prescribed, and you will be told when you can start moving your toes and ankle.
Prevention
Wear insoles and well-fitting shoes to help slow down the progression of bunions and alleviate discomfort. Cushioning can also help alleviate discomfort. Consider wearing shoes with a wide toe box so they don't crowd your toes. Children can also develop bunions and should wear properly fitting shoes as their feet are still developing.
Study Overpronation
Overview
Overpronation represents a dysfunction in the biomechanics of the body, and it is not a disease. Occasionally it may make your feet ache, but it need not be that much of a problem. If you wear comfortable shoes for overpronation such as stability shoes or motion control shoes for running, that is all that is needed in most cases to prevent foot problems from developing. If you overpronate to a high degree, you may need orthopaedic devices for your shoes which will ensure the maximum amount of correction.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding additional stress to other parts of the foot. Therefore over-pronation can often lead to a case of Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. People with flat feet often do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
When you overpronate your foot rolls inwards causing the lower leg to rotate inwards too. It's thought that this increases stress on the soft tissues of the lower leg causing pain and inflammation, or more commonly known as shin splints.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Overpronation represents a dysfunction in the biomechanics of the body, and it is not a disease. Occasionally it may make your feet ache, but it need not be that much of a problem. If you wear comfortable shoes for overpronation such as stability shoes or motion control shoes for running, that is all that is needed in most cases to prevent foot problems from developing. If you overpronate to a high degree, you may need orthopaedic devices for your shoes which will ensure the maximum amount of correction.
Causes
Over-pronation is very prominent in people who have flexible, flat feet. The framework of the foot begins to collapse, causing the foot to flatten and adding additional stress to other parts of the foot. Therefore over-pronation can often lead to a case of Plantar Fasciitis, Heel Spurs, Metatarsalgia, Post-tib Tendonitis and/or Bunions. There are many causes of flat feet. Obesity, pregnancy or repetitive pounding on a hard surface can weaken the arch leading to over-pronation. People with flat feet often do not experience discomfort immediately, and some never suffer from any discomfort at all. However, when symptoms develop and become painful, walking becomes awkward and causes increased strain on the feet and calves.
Symptoms
Common conditions that develop with prolonged overpronation typically include plantar fasciitis, achilles tendonitis, shin splints, posterior tibial stress syndrome and even IT band syndrome. With long term neglect you may see the development of bunyons, foot deformities and early onset of hip and knee arthritis.
Diagnosis
When you overpronate your foot rolls inwards causing the lower leg to rotate inwards too. It's thought that this increases stress on the soft tissues of the lower leg causing pain and inflammation, or more commonly known as shin splints.
Non Surgical Treatment
An overpronator is a person who overpronates, meaning that when walking or running their feet tend to roll inwards to an excessive degree. Overpronation involves excessive flattening of the arches of the feet, with the roll seeing the push off take place from the inside edge of the foot and the big toe. When this happens, the muscles and ligaments in the feet are placed under excessive strain, which can lead to pain and premature fatigue of the foot. Overpronation is most commonly experienced in people who have flat feet or fallen arches.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.